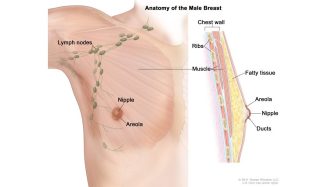
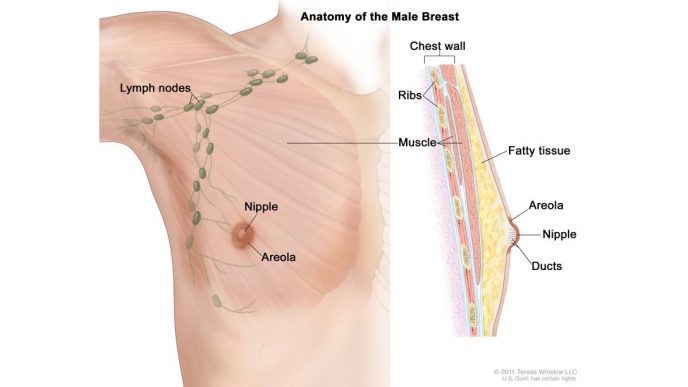
Health Politics Top Posts Citing Trump order on ‘biological truth,’ VA makes it harder for male veterans with breast cancer to get coverage byProPublicaNovember 3, 2025
Politics Riverside County Top Posts Biden signs bill to designate Sy Kaplan VA Clinic in Palm Desert byCity News Service Inc.December 20, 2022